Speech Sound Disorders
Lisp Speech Therapy — Types, Causes and Treatment

- There are four main types of lisp — interdental, dentalized, lateral, and palatal — each requiring different treatment approaches
- Mild frontal lisps in children under five may resolve naturally — lateral and palatal lisps almost never do
- Lisp speech therapy is highly effective at any age — adults achieve significant improvement with structured treatment
- Most children with a lisp complete treatment within three to six months of consistent weekly therapy
- Home practice between sessions is one of the strongest predictors of faster progress
- What is a lisp?
- The four types of lisp — with examples
- What causes a lisp?
- Age guidelines — when to seek help
- How lisp speech therapy works
- How long does treatment take?
- At-home practice strategies
- Common myths about lisps
- Frequently asked questions
What Is a Lisp?
A lisp is an articulation disorder that affects how the /s/ and /z/ sounds are produced. Instead of a clear, crisp sound, speech may come out distorted, muffled, or sound like “th.”
Lisps are speech production issues — not language problems. A child with a lisp typically understands language well and communicates effectively. The difficulty is specifically with the motor placement of the tongue during certain sounds.
Lisps are among the most common speech sound disorders seen in clinical practice — and among the most responsive to structured speech therapy. The key is identifying which type of lisp is present, because each type involves different tongue placement and requires a different treatment approach.
The Four Types of Lisp — With Examples
Identifying the correct type of lisp is the essential first step. A qualified speech-language pathologist will conduct a formal evaluation to determine which type is present before developing a treatment plan.
Interdental Lisp (Frontal Lisp)
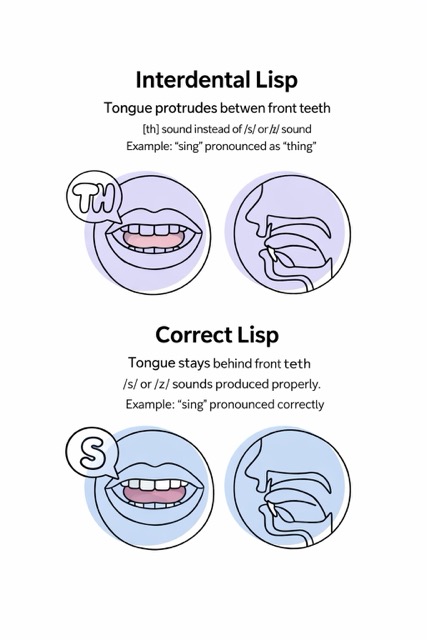
In an interdental lisp the tongue protrudes between the front teeth when producing /s/ and /z/ sounds. This produces a “th” sound instead of a clear /s/.
“Sing” sounds like “thing” — “sun” sounds like “thun”
This is the most common type of lisp in young children. It is also the most likely to resolve naturally in children under five. Persistent cases after age five or six should be evaluated by an SLP.
✓ May resolve naturally before age 5
Dentalized Lisp
In a dentalized lisp the tongue pushes against the back of the front teeth rather than resting just behind them in the correct position. The resulting sound is dull or muffled rather than sharp and crisp.
/s/ sounds flat and imprecise — lacking the sharp clarity of a correctly produced sound
A dentalized lisp is often subtle and may be overlooked. It typically requires guided correction to retrain proper tongue placement and does not resolve on its own.
✕ Requires therapy — does not resolve naturally
Lateral Lisp
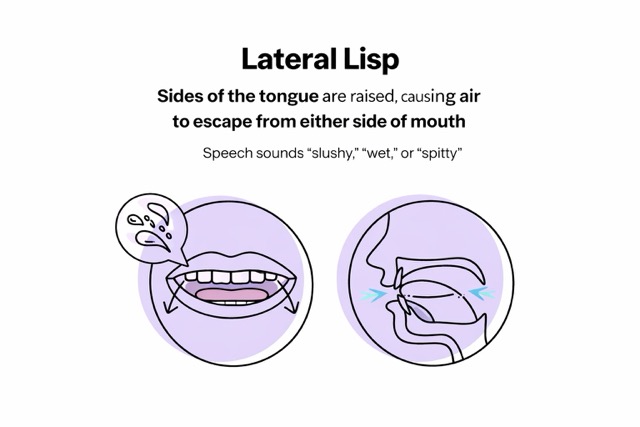
A lateral lisp occurs when air escapes over the sides of the tongue instead of flowing directly down the centre. This produces a distinctive “wet,” “slushy,” or “spitty” sound quality that is immediately noticeable to listeners.
/s/ and /z/ sounds have a wet, slushy quality — often described as sounding like the speaker has saliva in their mouth
Lateral lisps are the most socially noticeable type and the most likely to affect a child’s confidence and willingness to speak. They almost never resolve without direct speech therapy intervention.
✕ Requires therapy — rarely resolves without intervention
Palatal Lisp
In a palatal lisp the tongue makes contact with the soft palate — the roof of the mouth — too far back. This produces a distorted /s/ or /z/ that sounds unclear or unusual.
/s/ sounds distorted with a quality that is difficult to describe precisely — but immediately noticeable as different from a typical /s/ sound
Palatal lisps are less common than the other three types but almost always require structured speech therapy. This type does not resolve naturally.
✕ Requires therapy — does not resolve naturally
What Causes a Lisp?
Lisps develop when the tongue habitually moves to an incorrect position during speech. Over time these patterns become automatic and feel natural to the speaker — even though they produce distorted sounds. Several factors can contribute to or reinforce incorrect tongue placement.
The most common cause. The tongue develops an incorrect resting or movement pattern that becomes automatic over time.
Extended thumb or finger sucking can push the tongue forward and alter dental arch shape, contributing to frontal lisps.
A swallowing pattern where the tongue pushes forward against or between the teeth — reinforcing frontal tongue placement during speech.
An open bite or other dental differences can make correct tongue placement physically more difficult during sound production.
Children who cannot hear speech clearly may develop inaccurate sound production patterns including lisps.
Children sometimes model the speech of family members or caregivers who lisp — learning the pattern as their default.
Lisps are motor speech patterns — not signs of laziness, low intelligence, or lack of effort. They reflect how the tongue has learned to move, not how hard someone is trying to speak correctly. This is an important distinction for parents and adults seeking treatment.
Age Guidelines — When to Seek Help
One of the most common questions parents ask is whether their child will outgrow a lisp. The answer depends on the type of lisp and the child’s age. Here are clear guidelines based on developmental norms.
If a child avoids speaking, appears frustrated when communicating, or is being teased by peers, early support is warranted regardless of age. The emotional impact of a lisp can be significant — and addressing it early protects confidence during critical developmental years.
Adults with lisps should also consider an evaluation. It is never too late to improve articulation — adults regularly achieve significant improvement with structured lisp speech therapy.
How Lisp Speech Therapy Works
Lisp speech therapy is a systematic, goal-oriented process that retrains the tongue to move correctly during sound production. The approach varies depending on the type of lisp but follows a consistent progression from awareness to automatic use in everyday speech.
-
1Comprehensive evaluation
The SLP identifies the specific type of lisp, assesses tongue placement, evaluates airflow direction, and documents how the lisp affects connected speech. This determines the treatment approach. -
2Awareness training
The child or adult learns to feel and hear the difference between incorrect and correct tongue placement. Mirrors, tactile cues, and audio recordings are commonly used at this stage. -
3Sound production in isolation
The correct /s/ or /z/ sound is practised in isolation — just the sound itself — until it can be produced accurately and consistently before progressing. -
4Syllables and words
The correct sound is practised in syllables, then words — first at the beginning of words, then the middle, then the end. Each position is practised until consistent before moving on. -
5Sentences and conversation
The correct sound is practised in phrases, sentences, and eventually natural conversation. This stage requires the most time — the goal is automatic correct production without conscious effort. -
6Carryover into daily speech
Strategies are practised to generalise correct production across all environments — home, school, work, and social situations. Home practice is essential at this stage.
How Long Does Lisp Speech Therapy Take?
Treatment duration varies by type of lisp, age, consistency of practice, and how long the incorrect pattern has been established. As a general guide:
| Lisp type | Typical duration | Key factors |
|---|---|---|
| Interdental (frontal) | 3–6 months | Responds well — especially in children under 8. Daily home practice accelerates progress significantly. |
| Dentalized | 2–4 months | Often resolves relatively quickly with targeted tongue placement work. |
| Lateral | 6–12 months | More complex pattern to retrain. Requires patience and consistent therapy — but highly treatable. |
| Palatal | 6–12 months | Less common — requires specialist expertise. Duration varies based on severity. |
| Adults — any type | 3–9 months | Adults are highly motivated and often progress efficiently. Long-established patterns may take longer to retrain. |
These are general ranges. Some children make remarkable progress in just a few months of weekly therapy with strong home practice. Others with more complex needs or longer-established patterns may take longer. Your SLP will provide a more specific estimate after the initial evaluation.
At-Home Practice — What Makes the Biggest Difference
What happens between sessions is as important as what happens during them. The SLP sets the direction and teaches the technique — but it is the daily repetition at home that builds the new muscle memory that makes correct speech automatic.
Five minutes of focused daily practice at home consistently produces faster results than weekly therapy alone. Short, frequent practice beats occasional long sessions. The goal is repetition — making the correct tongue position feel natural through sheer volume of practice in a low-pressure environment.
Practical home practice strategies that work:
- Short daily sessions — 5 to 10 minutes is enough and sustainable
- Practise only the specific targets the SLP has assigned — not random sounds
- Use a mirror so the child can see their own tongue placement
- Positive reinforcement — celebrate correct productions, not just effort
- Avoid constant correction during natural conversation — this causes anxiety and avoidance
- Set a specific practice time each day — consistency matters more than duration
Common Myths About Lisps
Frequently Asked Questions
Related Guides
Ready to find a lisp speech therapist?
Browse our directory of ASHA-certified speech-language pathologists by state — including specialists in articulation and lisp treatment for children and adults.
Always consult a licensed speech-language pathologist for evaluation and treatment recommendations.
© 2026 Burke Networks · Editorial Policy